


































 Time:Feb 03, 2026
Time:Feb 03, 2026
 Share:
Share:


“ For one week before my period, I feel like a completely different person. ”
This experience is widely shared among women. Low mood, irritability, breast tenderness, headaches, sleep disturbances, difficulty concentrating, water retention, and increased appetite are often perceived as “normal” premenstrual discomfort.
In reality, these symptoms are characteristic features of premenstrual syndrome (PMS), while more severe and persistent manifestations may meet the diagnostic criteria for premenstrual dysphoric disorder (PMDD). [1]
Epidemiological data show that premenstrual symptoms are far more prevalent than commonly assumed. Globally, up to 90% of women experience at least one premenstrual symptom, approximately 20–30% meet the criteria for PMS, and 2–5% develop symptoms severe enough to be classified as PMDD. [2]

PMS/PMDD: A Growing Pain Point for Young Women
For many women, the week before menstruation can feel physically and emotionally overwhelming. Common complaints include mood changes, irritability, fatigue, sleep disturbances, and difficulty concentrating. While often normalized, these symptoms can significantly affect daily life, work performance, and relationships.
What Is PMS and PMDD?
PMS refers to a group of recurring physical and emotional symptoms that occur during the luteal phase of the menstrual cycle and resolve after menstruation begins. PMDD is a more severe form, characterized by pronounced emotional and psychological symptoms that can interfere with normal functioning.
PMS Symptoms
Mood swings
Irritability
Fatigue
Breast tenderness
Headaches
Bloating
Sleep disturbances
PMDD Symptoms
Persistent low mood or depression
Anxiety or tension
Anger or irritability
Emotional sensitivity
Difficulty concentrating
Compared with PMS, PMDD symptoms are more intense and often require targeted intervention. [1]
How Do Supplements for PMS and PMDD Work?
Most supplements for PMS aim to support hormonal balance, neurotransmitter regulation, or stress response pathways. Common mechanisms include:
Modulating estrogen activity
Supporting serotonin signaling linked to mood regulation
Reducing inflammation and oxidative stress
Stabilizing hormonal fluctuations during the luteal phase
However, not all supplements address the root causes of individual hormonal sensitivity—one reason why responses vary widely among women.
Why Consider S-Equol in PMS Support Formulations?
When S-equol is mentioned, it is often associated with menopausal health, including support for hot flashes, bone health, and cardiovascular function. Less widely recognized is that emerging research suggests the potential relevance of S-equol may extend beyond menopause, indicating possible benefits for premenstrual health in younger women.
New Clinical Evidence: S-Equol Producers Have a Lower Risk of Premenstrual Distress
For many years, clinical approaches to managing premenstrual syndrome and premenstrual dysphoric disorder (PMS/PMDD) have shown clear limitations. Commonly used oral contraceptives may help alleviate certain symptoms by modulating hormone levels, but are often associated with side effects such as menstrual irregularities, weight gain, and mood fluctuations.
Selective serotonin reuptake inhibitors (SSRIs) may also cause adverse effects including nausea and dizziness, leading many women to discontinue or avoid these interventions [3]. As a result, identifying safe and effective non-pharmaceutical strategies has become a key focus of clinical research.
A 2026 clinical study conducted at Ochanomizu University in Japan recruited 42 healthy young Japanese women aged 19–20. Participants were classified as equol producers or non-producers based on urinary equol concentrations (≥0.1 μM), and PMS/PMDD severity was assessed using standardized questionnaires. The results were notable: among individuals with moderate-to-severe PMS/PMDD, the proportion of equol producers was significantly lower than that of non-producers (p < 0.05). Although exploratory and limited by sample size, this study suggests a potential role for equol in modulating premenstrual symptoms in young women. [4]
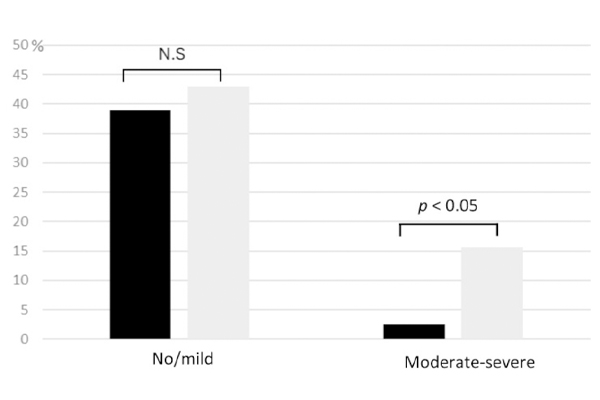
Figure 1. Distribution of s-equol production status across PMS/PMDD severity levels.
Black bars represent s-equol producers; grey bars represent non-producers.
Earlier Studies Also Support the Link Between S-Equol and Premenstrual Outcomes
Multiple observational and interventional studies further support the link between equol and premenstrual health:
2016 cross-sectional study (women 20–45): equol producers were more common among healthy participants (41.8%) than among women with PMS (23.9%), and the difference was statistically significant (P < 0.05). [5]
2018 cross-sectional study (Japanese collegiate female athletes, 18–21): 54.5% reported premenstrual symptoms interfering with training or competition performance; further analysis indicated that being unable to produce equol was a significant risk factor (OR = 3.34). [6]
2022 open-label pilot intervention (19 PMS patients, all non-producers): participants took 5 mg/day of S-equol starting on day 5 of the menstrual cycle for two consecutive cycles; 10.5% achieved a 50% reduction in DRSP score, and key PMDD core symptoms—depression, anxiety, irritability, and mood swings—showed significant improvement. [7]
Together, these findings position S-equol as a promising, evidence-based ingredient in supplements for PMS mood swings and PMDD support.
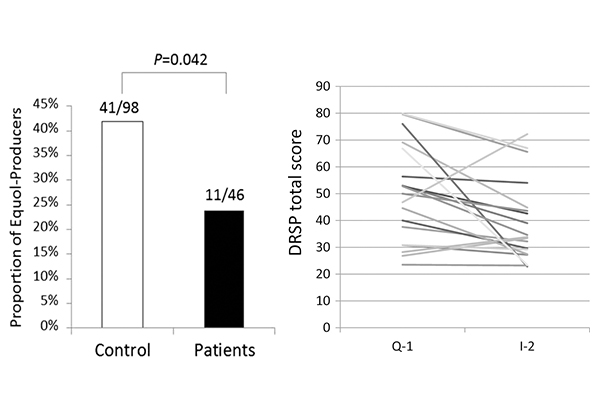
Figure 2. S-equol production status and PMS-related symptom scores.
Left panel shows the proportion of equol producers among healthy individuals and PMS patients; right panel shows DRSP scores before and after S-equol supplementation.
Safety Profile of S-Equol
S-equol has been extensively studied for safety and tolerability. Human clinical data show that S-equol supplementation is well tolerated, with no serious adverse effects reported at commonly used doses.
For brands and consumers alike, safety assessments and regulatory evaluations—such as GRAS determinations—provide additional confidence when incorporating S-equol into long-term wellness routines.
(Learn more in our detailed S-equol safety overview.)
S-Equol–Rich Foods: Why Diet Alone Is Often Not Enough
S-equol is not naturally present in most foods. Instead, it is produced in the gut when specific intestinal bacteria metabolize soy isoflavones, particularly daidzein.
However, only a portion of the population, often less than 40 percent, can naturally produce equol. For non-producers, consuming soy foods alone does not result in meaningful S-equol exposure, making direct supplementation the only reliable option.
Although S-equol itself does not occur naturally in foods, certain dietary components can provide precursors or create a gut environment that supports its formation:
Soybeans and soy products
Including soybeans, tofu, soy milk, natto, and miso. These foods are rich in soy isoflavones, especially daidzein, the direct precursor of S-equol. Regular intake supplies the necessary substrate for equol-producing gut bacteria.iber-rich foods
Such as whole grains, vegetables, fruits, and nuts. Dietary fiber supports gut microbiota balance and intestinal function, helping maintain bacterial populations capable of converting soy isoflavones into S-equol.Cruciferous vegetables
Including broccoli, cabbage, radish, and kale. These vegetables contain glucosinolates that are metabolized by gut microbes into bioactive compounds, indirectly supporting a microbiome environment favorable for S-equol production.

Despite these dietary strategies, individual differences in gut microbiota mean that many people remain non-producers, even with long-term dietary intervention.
Who Else Should Consider S-Equol?
Beyond young women experiencing PMS or PMDD symptoms, S-equol may also be relevant for broader populations across different hormonal life stages—consistent with previous clinical research and applications.
S-equol has been most extensively studied in perimenopausal and postmenopausal women, where it has demonstrated benefits related to vasomotor symptoms, bone health, and overall hormonal balance. As such, women transitioning from reproductive age into perimenopause may find S-equol particularly relevant during periods of increasing hormonal variability.
References
[1] Henshaw C A. PMS: diagnosis, aetiology, assessment andmanagement: Revisiting… Premenstrual syndrome [J]. Advances in Psychiatric Treatment, 2007, 13(2): 139-46.
[2] Yang Y, Jia Y, Fu S, et al. The prevalence of premenstrual syndrome in China: a systematic review and meta-analyses [J]. Frontiers in psychiatry, 2025, 16: 1640781.
[3] Management of Premenstrual Disorders: ACOG Clinical Practice Guideline No. 7 [J]. 2023, 142(6): 1516-33.
[4] Kada-Kondo N, Kimura N, Isobe K, et al. Urinary Equol Production Capacity, Dietary Habits, and Premenstrual Symptom Severity in Healthy Young Japanese Women [J]. Metabolites, 2026, 16(1).
[5] Takeda T, Ueno T, Uchiyama S, et al. Relation between premenstrual syndrome and equol-production status [J]. 2016, 42(11): 1575-80.
[6] Takeda T, Ueno T, Uchiyama S, et al. Premenstrual symptoms interference and equol production status in Japanese collegiate athletes: A cross-sectional study [J]. 2018, 44(3): 488-94.
[7] Takeda T, Chiba Y. Evaluation of a natural S-equol supplement in treating premenstrual symptoms and the effect of the gut microbiota: An open-label pilot study [J]. 2022, 42(2): 127-34.










 +1(425)866-9043
+1(425)866-9043
 sales@bonerge.com
sales@bonerge.com