


































 Time:Apr 15, 2026
Time:Apr 15, 2026
 Share:
Share:


GLP-1 receptor agonists such as semaglutide and tirzepatide are revolutionizing weight management and metabolic health. The global market for these drugs reached USD 66.38 billion in 2025, and it will grow to USD 185.32 billion by 2033, with an annual growth rate of 12.4%. These medications have become core treatments for type 2 diabetes and obesity.[1]
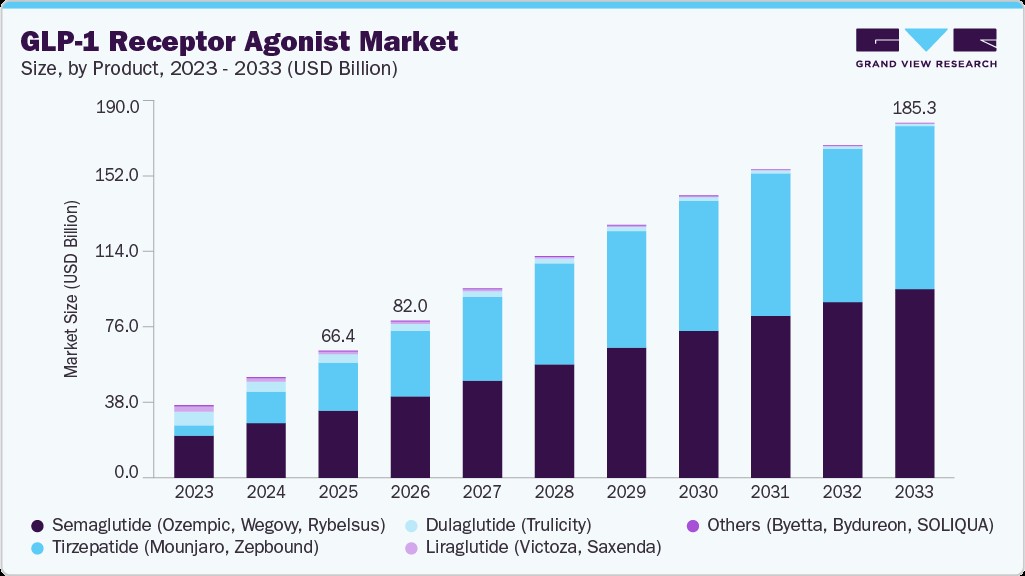
Figure 1: GLP-1 Receptor Agonist Market Size by Product, 2023–2033 (USD Billion). Source: Grand View Research [1]
These drugs boost insulin secretion, halt glucagon release, slow gastric emptying, and help people feel full faster. Yet these therapies do not work in a nutritional vacuum. Patients eat far less, so they commonly face significant nutritional gaps. The supplement industry can effectively help these users meet their nutritional needs.
The GLP-1 companion supplement segment is one of the most promising emerging categories in functional nutrition. This article explains GLP-1 drug physiology, the nutritional gaps these users face, and evidence-based ingredient strategies for product development.
Why GLP-1 Users Need Nutritional Support
GLP-1 receptor agonists mainly slow gastric emptying, strengthen satiety signals in the brain, and reduce the reward response to high-calorie foods.[2] These effects lead to consistent, meaningful reductions in food intake.
When total calorie intake drops sharply, getting enough protein, fiber, vitamins, and minerals becomes structurally difficult—not just a matter of willpower.
GLP-1 users often face these key nutritional issues:
Protein insufficiency: Reduced appetite cuts total calorie intake sharply. Without intentional planning, protein intake often falls below the level needed to preserve muscle during weight loss.
Micronutrient shortfalls: Smaller food portions mean lower intake of B vitamins, magnesium, zinc, iron, and other key micronutrients.
Reduced fiber intake: Fiber-rich foods are filling. GLP-1 users with smaller meals typically eat less fiber, which worsens gastrointestinal side effects—especially constipation—caused by GLP-1 drugs.
Lean mass loss: Body composition data from GLP-1 trials shows 25% to 40% of weight lost during treatment comes from lean mass, not fat.[3] This harms long-term metabolic rate, physical function, and weight maintenance after stopping treatment.
The Lean Mass Problem
Skeletal muscle is metabolically active tissue. It supports resting energy expenditure and glucose processing. Losing muscle during weight loss undermines long-term health.
Clinical guidelines advise GLP-1 users to prioritize sufficient dietary protein—usually 1.2–1.6 g per kilogram of body weight daily or more—and regular resistance training to trigger muscle protein synthesis.[3]
These steps are hard to follow in practice. A reduced appetite makes it tough to hit protein goals with whole foods alone. Many users also do not exercise consistently, especially early in treatment.
This gap creates a clear need for high-quality protein supplements designed for GLP-1 users: small portions, easy digestion, and optimized amino acid profiles with sufficient leucine.
Key Ingredient Categories
1. Protein
Protein is the foundation of any glp1 supplement or glp 1 nutrition companion. The main challenge is delivering complete protein in portions that work with suppressed appetite.
Whey protein isolate and concentrate are the most researched choices for supporting muscle protein synthesis. They contain about 10–11% leucine in their amino acid profile and digest quickly, so they effectively stimulate muscle protein synthesis even in a calorie deficit.[4]
Plant-based blends (such as pea + rice protein) provide a complete amino acid profile. They serve the growing number of GLP-1 users who want non-dairy options.
Collagen peptides are popular but not a complete protein and low in leucine. You should not use collagen as the main protein source for glp-1 lean mass preservation.
2. Dietary Fiber
Fiber serves two key roles for glp 1 support: it supports gut motility to reduce constipation risk, and soluble fiber stabilizes blood sugar and boosts satiety.
Well-tolerated, clinically supported soluble fiber options include partially hydrolyzed guar gum (PHGG), inulin, and psyllium husk.
Important formulation note: Fermentable fibers can worsen bloating and GI discomfort in users already dealing with drug-related side effects. Both fiber type and dosage matter.
3. Essential Micronutrients
Key nutrients for GLP-1 users include:
B vitamins (B12, B6, folate): Support energy metabolism and nerve function
Magnesium: Aids muscle function, sleep, and blood sugar control
Iron & zinc: Choose chelated forms for better absorption with low food intake
Vitamin D & K2: Support bone and heart health
4. Gut Health and the GLP-1 Connection
Gut health is a critical part of glp 1 nutrition support. GLP-1 is a gut hormone made by intestinal L-cells, and gut microbiome balance directly affects how much GLP-1 the body produces naturally.
Akkermansia muciniphila is the most studied ingredient in this space. It releases a P9 protein that binds to intestinal L-cell receptors and stimulates GLP-1 secretion in a calcium-dependent way.[5]
Beyond boosting GLP-1, Akkermansia also slows gastric emptying and reduces appetite to support weight management.[5]
Amuctive™ Akkermansia is a next-generation innovation that focuses on the Amuc_1100 protein. The name stands for "Amuc" plus "Active" to highlight this essential active component. This product uses patented enrichment and detection technology to achieve Amuc_1100 levels over three times higher than conventional Akkermansia products. It is SA-GRAS certified and backed by more than 10 global patents for its production and formulation processes.
Preclinical studies show that Amuctive™ helps reduce weight regain after stopping semaglutide. It also helps improve glycemic markers during this transition period. These benefits make it a very relevant ingredient for supplements targeting the post-GLP-1 market. This ingredient offers a safe and scientifically validated way to maintain metabolic health.

5. Berberine and Dihydroberberine
Berberine strongly supports GLP-1 secretion. It increases proglucagon mRNA expression and L-cell growth to raise GLP-1 output. It also activates the gut’s TAS2R38 bitter taste receptor, which directly triggers GLP-1 secretion in a dose-dependent way.[7]
Dihydroberberine (DHB) is the more bioavailable form of berberine. The body quickly converts absorbed DHB to berberine for full effects.
DHB also improves insulin resistance. When insulin resistance exists, GLP-1 works less well to control blood sugar. Better insulin sensitivity makes GLP-1 drugs more effective.[8] DHB also has anti-inflammatory effects that may ease inflammation-related side effects of GLP-1 medications.[8]
Formulation Considerations
Product format is critical for supplements for glp-1 users. These users have smaller appetites and may feel nauseous or have GI discomfort, especially early in treatment.
Practical design rules:
Use compact, high-nutrient-density formats: protein shakes, stick packs, and small capsules work better than large tablets or big powder servings
Account for changed taste and smell sensitivity with GLP-1 use
Spread protein intake throughout the day and time supplements around activity
Make small-portion products: a 150–200 ml serving with 20+ g protein is more realistic than a 400 ml shake
The Market Opportunity
30–50 million Americans may join the GLP-1 market in coming years. Discontinuation rates are very high—up to 83% in some studies—due to cost, side effects, and weight-loss plateaus.[9] Studies show many users regain two-thirds of lost weight within a year of stopping treatment.[10]
This creates two large markets: nutrition support during GLP-1 use, and metabolic maintenance after stopping treatment.
Brands, formulators, and private-label manufacturers that build science-backed glp 1 nutrition companion products now will lead this category, which will shape functional nutrition for the next decade.

Conclusion
GLP-1 receptor agonists have changed how millions manage weight and metabolic health. They create predictable nutritional challenges that the right supplements can solve.
The four pillars of a strong GLP-1 companion strategy are:
glp-1 lean mass preservation
Gut microbiome support
Adequate protein intake
Complete micronutrient coverage
Effective ingredients exist, and science supports their use. The key is to combine them in formats that fit the real needs of GLP-1 users.
References:
[1] Grand View Research. GLP‑1 receptor agonist market size, share & trends analysis report 2026–2033[EB/OL]. (n.d.)[2026-04-15]. https://www.grandviewresearch.com/industry-analysis/glp-1-receptor-agonist-market.
[2] Müller TD, et al. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov. 2022;21(3):201-223.
[3] Sargeant JA, et al. Changes in lean body mass with glucagon-like peptide-1-based therapies and mitigation strategies. Obes Rev. 2024;25(8):e13752.
[4] Gorissen SHM, et al. Protein content and amino acid composition of commercially available plant-based protein isolates. Amino Acids. 2018;50(12):1685-1695.
[5] Niu H, Zhou M, et al. Molecular Mechanism of Pasteurized Akkermansia muciniphila in Alleviating Type 2 Diabetes Symptoms. J Agric Food Chem. 2024;72(23):13083-13098.
[6] Plovier H, et al. A purified membrane protein from Akkermansia muciniphila or the pasteurized bacterium improves metabolism in obese and diabetic mice. Nat Med. 2017;23(1):107-113.
[7] Yang WL, Zhang CY, et al. Berberine Metabolites Stimulate GLP-1 Secretion by Alleviating Oxidative Stress and Mitochondrial Dysfunction. Am J Chin Med. 2024;52(1):253-274.
[8] Li C, Dong N, Wu B, et al. Dihydroberberine, an isoquinoline alkaloid, exhibits protective effect against dextran sulfate sodium-induced ulcerative colitis in mice. Phytomedicine. 2021;90:153631.
[9] Weiss T, et al. Real-world persistence and adherence to glucagon-like peptide-1 receptor agonists among obese commercially insured adults without diabetes. J Manag Care Spec Pharm. 2024;30(5):439-448.
[10] Wilding JPH, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564.








 +1(425)866-9043
+1(425)866-9043
 sales@bonerge.com
sales@bonerge.com